We often get asked: “Can I have both?” — short answer: yes. But let’s start slow and clear.
Quick definitions — astigmatism vs myopia
What is myopia (nearsightedness)?
Myopia means you see nearby objects clearly but distant objects are blurry. Think of it like a camera whose focus is set too close — distant scenes land out of focus on the retina. Usually this happens when the eyeball is a bit too long or the cornea has too much curvature for the eye’s length.
What is astigmatism?
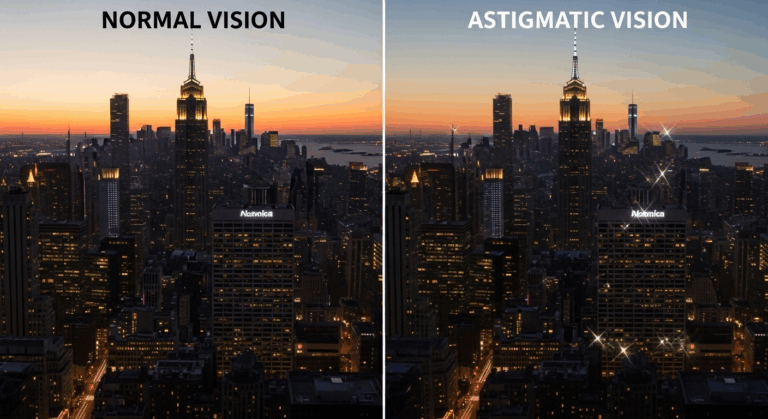
Astigmatism is when the eye’s front surface (cornea) or lens is shaped more like a football than a perfect round soccer ball. That uneven curvature bends light differently in different meridians, producing stretched or distorted vision at all distances — lines may look tilted, doubled, or fuzzy.
How they affect vision — side-by-side
Visual symptoms of myopia

- Blurry distance vision (road signs, TV, the whiteboard in class).
- Headaches and eye strain after trying to focus far away.
- You might bring things closer to focus on small text or distant objects.
Visual symptoms of astigmatism

- Blurred or distorted vision at near and far.
- Difficulty reading fine print; letters may appear stretched or shadowed.
- Squinting often helps temporarily — it changes the eye’s aperture and can reduce blur.
Overlap and mixed cases
It’s common to have both. For example, you might be nearsighted but also have astigmatism, which means distance objects are blurry and everything may have a slight “wobble” or double-edge.
Causes and risk factors
What’s behind myopia?
- Genetic tendency — it often runs in families.
- Environmental factors — lots of close work or limited outdoor time in childhood is associated with earlier onset and progression.
- Eye growth — the eye elongates during development.
What’s behind astigmatism?
- Irregular corneal curvature (most common).
- Lens irregularities or scars (less common).
- Can be present from birth or follow eye injury or surgery.
Remember: having one doesn’t rule out the other. We often see patients who assume they “only” have myopia, then discover a mild astigmatism on exam that explains remaining blur.
Diagnosis — how eye care pros tell them apart
Eye chart and visual acuity test
Standard Snellen or digital charts can show reduced distance acuity (myopia) and patterns of blur, but they’re not the whole story.
Refraction (objective and subjective)
- Objective refraction: instruments like autorefractors and retinoscopy estimate how light focuses in your eye.
- Subjective refraction: “Which is better — 1 or 2?” — lets the clinician fine-tune lenses. Astigmatism is detected by testing different cylinder powers and axes.
Keratometry and corneal topography
These map corneal shape. If the cornea is toric (football-shaped), corneal topography will show it clearly — very helpful for diagnosing astigmatism.
Treatment & correction options (general overview)
I’m going to keep this high-level — it’s important to avoid giving medical instructions without a personal exam. That said, here are the common approaches people hear about.
Glasses
- The simplest, safest start. A single-vision lens corrects myopia; astigmatism needs a cylindrical component (axis + power) in the prescription.
- Glasses are adjustable and non-invasive — think of them as the default first step.
Contact lenses
- Soft spherical lenses correct myopia. Toric contact lenses correct astigmatism by having orientation-stable designs.
- Some people prefer contacts for sports or cosmetic reasons, but they require proper fit and care.
Refractive procedures
- Procedures (e.g., LASIK-like surgeries) change how the cornea focuses light. They can address myopia and astigmatism, sometimes together.
- Important: only an eye care professional can tell you if you’re a candidate after a thorough evaluation.
Monitoring and follow-up
Regular eye exams matter — especially for children (myopia can progress) and for anyone whose vision changes or who has headaches/eye strain.
Practical differences — how to spot which you (or someone you love) might have
Quick checklist
- Blurry only at distance = likely myopia.
- Blurry at all distances, or letters look stretched/ghosted = likely astigmatism.
- Squinting helps for both, but if squinting still leaves odd-shaped letters, astigmatism is suspect.
- Sudden changes in vision, flashes, floaters, or pain = see an eye doctor promptly (these are red flags).
Kids and vision
Kids might not say “I can’t see far” — they’ll sit close to the TV or hold books near. If a child shows learning or behavior changes, have their vision checked. Early detection prevents learning difficulties and supports eye development.
When to see an eye care professional
- If blur interferes with daily life (driving, school, work).
- If headaches or eye strain are chronic.
- For routine screening: adults every 1–2 years depending on risk; kids more frequently.
- Any sudden loss of vision, flashes, or pain — urgent evaluation needed.
Lifestyle tips and eye comfort

- Take breaks during prolonged near work — follow the 20-20-20 rule: every 20 minutes look 20 feet away for 20 seconds.
- Ensure good lighting when reading or working.
- For kids, balanced time outdoors is associated with lower myopia onset (we often recommend outdoor play for general eye health).
- Wear prescribed correction — straining to see makes tasks tiring and uncomfortable.
Conclusion
Astigmatism vs myopia: both can blur your world, but they blur it in different ways. Myopia mainly affects distance clarity; astigmatism distorts and blurs across distances because of an irregular curvature. The good news? Both are diagnosable and commonly corrected with glasses, contacts, or other professional options. Remember: the exact plan should come from an eye care professional after a proper exam. We often say — don’t guess, get tested.